
A-Fib Fact Sheet

Atrial Fibrillation: The New Epidemic in Cardio Disease1
Atrial Fibrillation (A-Fib or AF) is the most common cardiac arrhythmia (abnormal heart rhythm) seen by physicians. It is one of the most undertreated heart rhythm disorders in America and accounts for about one-third of hospital admissions.2
What is Atrial Fibrillation?
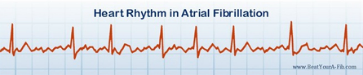
Atrial Fibrillation is a serious heart disease in which the upper chambers (atria) of the heart beat out of rhythm with the lower chambers (ventricles) of the heart. This causes the heart to race in an irregular and often rapid pattern, as fast as 300 to 600 times per minute (normal adult rate is 60–100 beats per minute).
- In A-Fib, you lose 15% or more of your heart’s normal pumping volume along with lower oxygen levels. Your body and brain aren’t getting the blood and nourishment they need.
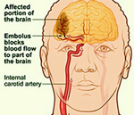
- A progressive disease, A-Fib can lead to other heart rhythm problems. When left untreated, A Fib patients have a five times higher chance of stroke, and a greater risk of heart failure.2
- A-Fib is often dismissed by doctors as a nuisance arrhythmia because it is not immediately life threatening. Nonetheless, atrial fibrillation sometimes requires emergency treatment and can lead to complications.
- Diagnosis is by a combination of taking the patient’s pulse and by a simple test called an electrocardiogram (ECG or EKG).
- What are the symptoms of Atrial Fibrillation?
- Symptoms can include pounding or fluttering in the chest (palpitations), shortness of breath, weakness, chest pain, fatigue, dizziness or fainting. Often patients feel tired and listless.
- Episodes of atrial fibrillation can come and go, or may be chronic; and can range from mild to severe. Some A-Fib patients feel no symptoms at all.
How many patients suffer from A-Fib?
- Estimates of Americans with atrial fibrillation vary from 2.7 million up to 6.1 million.
- By 2050 it’s estimated that number will rise to over 15.9 million.3
- About 500,000 new cases are diagnosed in the US per year.4
- Worldwide, there are about 600 million cases of Atrial Fibrillation.5
Who gets Atrial Fibrillation?
- Anyone can get A-Fib. But the older one becomes, the more likely A-Fib is to develop. Persons over the age of 40 have a 1 in 4 lifetime risk of developing atrial fibrillation.6
- A-Fib affects about 1 in 25 people aged 60 and older, and 1 in 10 people aged 80 and older.3
- Approximately 70 percent of A-Fib patients are between the ages of 65 and 85. 2
What causes A-Fib?
- In many patients, there is no apparent cause for A-Fib. In others, A-Fib may be related to coronary artery disease (CAD), thyroid disease, structural defects of the heart and its valves, lung disease or other medical conditions.
- Research has shown a strong correlation between Atrial Fibrillation and high blood pressure (hypertension), diabetes, sleep apnea syndrome and obesity.
- A-Fib can also run in families.
To learn about A-Fib Triggers, see A-Fib.com Causes
What are the risks associated with A-Fib?
Serious consequences include stroke, permanent heart damage, heart attack, heart failure and death.
- The morality rate for untreated A-Fib is about double that of patients with normal sinus rhythm.2 A-Fib contributes to more than 88,000 deaths annually.4
- A-Fib-related stroke accounts for 15% to 20% of all strokes, i.e., about 75,000 a year.7
- A-Fib strokes are more severe and disabling.8, 9 A-Fib patients recovering from a stroke have about a 50% higher risk of remaining disabled or handicapped compared to stoke patients without A Fib.10
- Remodeling: A-Fib can damage and weaken the heart over time. Electrical “remodeling” can change the shape and size of the heart. The heart becomes less efficient at pumping blood, making it work harder and harder over time. Heart remodeling is progressive and can become permanent.
- Dementia: A-Fib patients are 44% more likely to develop dementia. Younger A-Fib patients are at higher risk of developing dementia, particularly Alzheimer’s.11
How is A-Fib treated?
There are three components to the treatment of Atrial Fibrillation:
- Addressing the increased risk of blood clots and stroke
- Controlling the rhythm and rate of the heart to prevent enlargement, development of fibrosis and heart disease
- Treating the patient's often debilitating symptoms
There are a number of short-term and long-term treatments aimed at controlling or eliminating the abnormal heart rhythm associated with A-Fib.
- Drug therapy for stroke risk: Anticoagulants (blood thinners) are used to reduce the risk of stroke.
- Drug therapies for Atrial Fibrillation: Medications for the treatment of A-Fib are designed to control the heart rate (pulse), regain and maintain normal heart rhythm.
- While medication has been considered the first-line treatment for A-Fib, research indicates that 50% of patients fail drug therapy.3
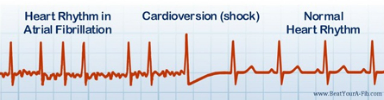
- Cardioversion delivers small, timed electrical shocks to the heart to restore 'normal sinus rhythm' (NSR). Though highly successful, only 23% of patients remain in normal sinus rhythm with most A-Fib recurring within one week.12
- Radiofrequency (RF) Catheter Ablation and CryoBalloon Ablation are minimally invasive catheter procedures that block electrical signals which trigger erratic heart rhythms. Success rates are 70%-85% for a single procedure and up to 90% with a second procedure.
- RF Catheter Ablation is the most common curative treatment worldwide for all types of A-Fib. Cryoablation is the newest treatment.
- Pacemakers may be implanted for pacing support, or in conjunction with Ablation of the
- AV Node.
- Surgery, classic Maze Surgery is open-heart, is usually performed today concurrent with other heart disease surgery. More common are the Mini-Maze surgeries (surgical ablation) through small port-size incisions in the chest. Success rates are 70%-85%.
For an in-depth discussion of Treatments, See A-Fib.com Treatments
What is the impact of Atrial Fibrillation?
- Treating A-Fib patients costs the U.S. about $26 billion annually, 4 which may in fact be an extremely low estimate. One study calculates that Medicare alone pays $15.7 billion per year to treat newly diagnosed A-Fib patients.13
- Hospital admissions caused by A-Fib accounts for about one-third of hospital admissions.2 A-Fib-related admissions have risen 60% in the last 20 years.14
- Patients with A-Fib often find that the normal activities of daily life become increasingly difficult and often have psychological, emotional and socials effects as well. Because A-Fib is a progressive condition, the patient’s quality of life often deteriorates.2
Additional Resources About Atrial Fibrillation

* Glossary of Atrial Fibrillation terms and phrases: see A-Fib.com Glossary http://a-fib.com/glossary/
* Free A-Fib graphics: see Graphics at BeatYourA-Fib.com online Press Room (samples at right)
* Pinterest: A-Fib Resources for journalists, writers, bloggers, and educators
* Atrial Fibrillation: Resources for Patients, since 2002, a non-profit website by a former A-Fib patient, www.A-Fib.com
* Atrial Fibrillation Association-US, branch of UK non-profit organization raising awareness of A-Fib; site includes patient education; http://www.atrialfibrillation-us.org/
* Heart Rhythm Society, world-wide association of cardiac arrhythmia professionals (cardiologists/electrophysiologists), patient education and advocacy; www.HRSonline.org

YYY
ABOUT THE AUTHOR: Steve S. Ryan, PhD, is publisher of the non-profit patient education website, Atrial Fibrillation: Resources for Patients, www.A-Fib.com, and author of the 5-star-rated book, Beat Your A-Fib: the Essential Guide to Finding Your Cure. Contact Dr. Ryan at ssryan@a-fib.com.
YYY
References
1 Atrial fibrillation: New management approaches for the "new epidemic" in cardiovascular disease. Joint report by The German Competence Network on Atrial Fibrillation (AFNET) and the European Heart Rhythm Association (EHRA), EHRA EUROPACE 2011, Madrid, Spain. 26 June, 2011. URL: http://tinyurl.com/AFib-Epidemic-Cardio-Disease
2 Fuster, V., Rydén, L. E., Cannom, D. S., et al. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial Fibrillation—Executive summary. Circulation 2006;114 (7), 700-752. doi: 10.1161/circulationaha.106.177031
3 Miyasaka Y, et al. Secular Trends in Incidence of Atrial Fibrillation in Olmsted County, Minnesota, 1980 to 2000, and Implications on the Projections for Future Prevalence. Circulation 2006; 114(2):119-125. http://circ.ahajournals.org/content/114/2/119.full
4 Kim, M. H., Johnston, S. S., Chu, B.-C., et al. Estimation of total incremental health care costs in patients with atrial fibrillation in the United States. Circulation: Cardiovascular Quality and Outcomes; 2011 2011;4:313-320. doi: 10.1161/CIRCOUTCOMES.110.958165
5 Camm, A. J., et al. Guidelines for the management of atrial fibrillation. European Heart Journal, 2010;31(19),2369-2429. doi:10.1093/eurheartj/ehq278
6 Lloyd-Jones, D.M, Wang TJ, Leip E, et al. Lifetime risk for development of atrial fibrillation. Circulation 2004;110:1042-1046. doi: 10.1161/01.CIR.0000140263.20897.42
7 Hart, R.G, Pearce, L.A, Rothbart, R.M, et al. Stroke with intermittent atrial fibrillation: incidence and predictors during aspirin therapy. Stroke Prevention in Atrial Fibrillation Investigators. J Am Coll Cardiol. 2000;35:183-187. URL http://view.ncbi.nlm.nih.gov/pubmed/10636278
8 Lin, H.J, Wolf, P.A, Kelly-Hayes, M, et al. Stroke severity in atrial fibrillation: the Framingham study. Stroke 1996;27:1760-4. URL http://view.ncbi.nlm.nih.gov/pubmed/8841325
9 Kelly-Hayes M, et al. The influence of gender and age on disability following ischemic stroke: The Framingham Study. J Stroke Carebrovasc Dis 2003; 12:119-26. doi: 10.1016/S1052-3057(03)00042-9
10 Lamassa M., et al. "Characteristics, Outcome, and Care of Stroke Associated with Atrial Fibrillation in Europe. Stroke. 2001; 32: 392-398 doi: 10.1161/01.STR.32.2.392
11 Bunch, T. Jared, and et al. "Atrial Fibrillation Is Independently Associated with Senile, Vascular, and Alzheimer's Dementia." Web. 1 Aug. 2011. doi: 10.1016/j.hrthm.2009.12.004
12 Boos C , More RS, Carlsson J. Persistent atrial fibrillation: rate control or rhythm control. BMJ 2003;326:1411–2. doi: 10.1136/bmj.326.7404.1411
13 Lee WC, et al. Direct treatment cost of atrial fibrillation in the elderly American population: a Medicare perspective. J Med Econ. 2008;11(2):281-98. doi: 10.3111/13696990802063425.
14 Friberg J, et al. Rising rates of hospital admissions for atrial fibrillation. Epidemiology. 2003 Nov;14(6):666-72. PubMed PMID: 1456918
YYY
Need a quote? or Subject matter expert?
Want A-Fib guests for your show or an article written?
Contact Steve S. Ryan, PhD at ssryan@a-fib.com,
310-266-7642 (cell) or 310-457-7126 (home office).
YYY
| Journalists, reviewers, bloggers and educators: You have our permission to post any of our informational documents, in whole or in part, as well as our photos and graphics on your website, blog, or in your print publication. We do ask that you include our website address and/or a link back to the Beat Your A-Fib website (www.BeatYourA-Fib.com). |
BACK TO PRESS ROOM
